Actuarial Medicine & Hidden Exclusion
How Hospitals Quietly Filter Out Complex Patients and Call It “Efficiency”

In insurer summits and hospital board meetings, administrators proudly tout “lower cost per patient,” “shorter hospital stays,” and “optimized bed usage.” At first glance, these metrics suggest streamlined, high-performing healthcare systems. But behind the polished numbers, a quieter reality unfolds—one that systematically excludes high-cost and complex patients before they ever appear in the data.
This phenomenon, which I call Actuarial Medicine, ensures that certain patients—older, disabled, low-income, uninsured—are steered away through algorithmic risk-scoring, bureaucratic friction, and anticipatory denial. By never formally rejecting them, hospitals lower their reported costs while shifting financial and human burdens elsewhere.
In this essay, I unpack how this hidden form of exclusion works, why hospitals use it, and what reforms are needed to ensure that “efficiency” isn’t just a euphemism for quietly abandoning those in need.
The Mechanics of Hidden Gatekeeping
a. The Rise of Algorithmic Risk Filtering
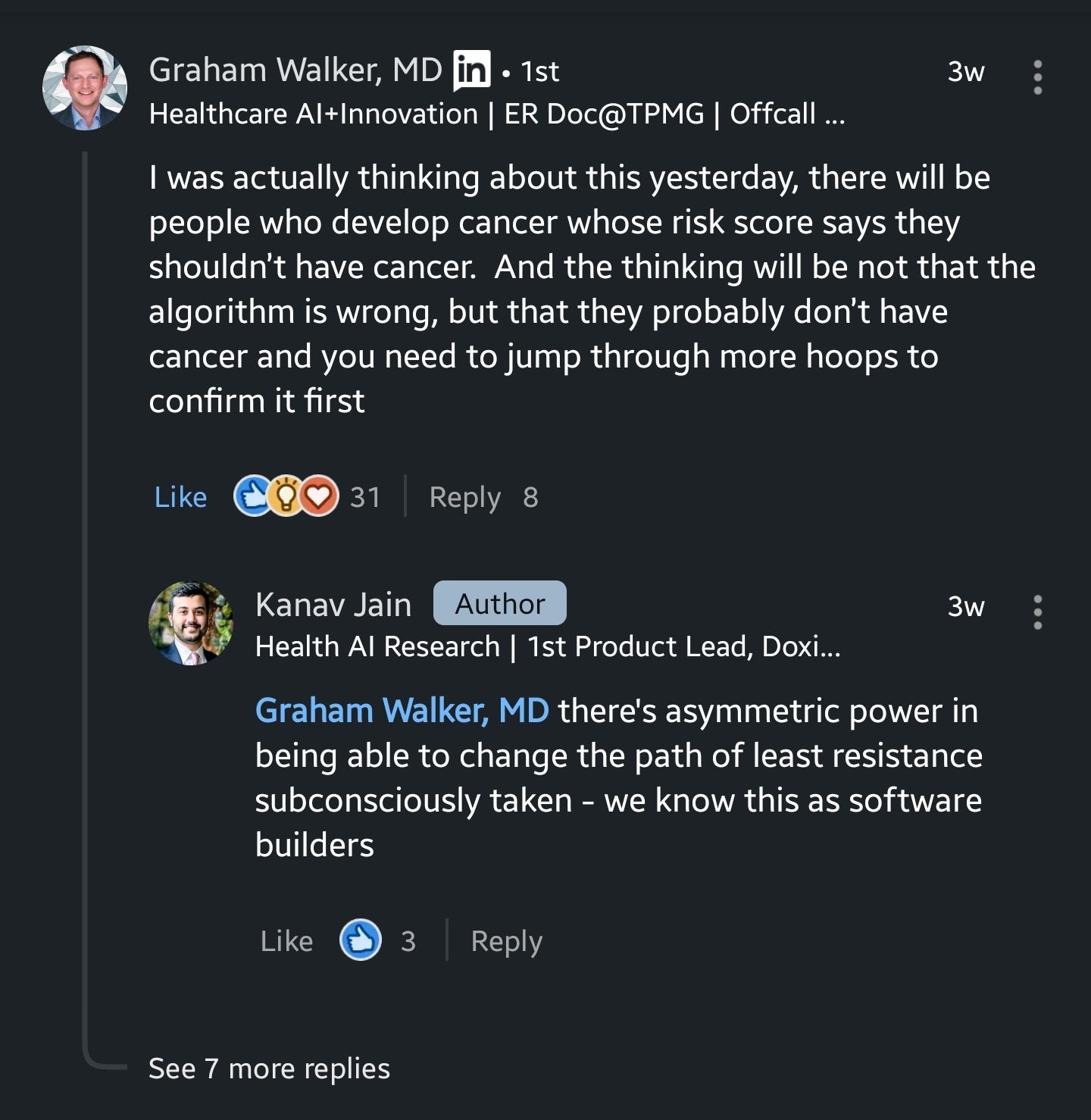
Hospitals increasingly rely on predictive analytics and risk-scoring software to assess whether a patient is “worth admitting.” These tools scan medical histories, insurance status, age, zip codes, and even socioeconomic indicators to assign risk scores. If flagged as high-cost, a patient may never receive an outright denial—instead, they encounter layers of subtle barriers.
Patients flagged as “complex” may face:
Coverage Re-checks: “Your insurance needs additional verification.”
Prior Authorizations: “You must complete further documentation before treatment.”
Triage Delays: “Your case needs secondary review; we’ll get back to you.”
Each step increases friction, creating attrition by exhaustion. The patient either gives up or experiences critical delays—yet officially, they were never denied.
Example: A 62-year-old woman with borderline diabetes and early cardiac symptoms is told her insurance needs additional verification. After weeks of unanswered calls and automated emails, she gives up. The hospital records her as “non-compliant,” not as a patient who needed care and was systematically deterred.
This form of anticipatory denial aligns with broader algorithmic austerity—where AI and data-driven systems quietly enforce rationing, optimizing for financial outcomes rather than human needs.
b. Administrative Burdens as a Screening Mechanism
Beyond AI-driven gatekeeping, hospitals weaponize bureaucracy to filter out “expensive” cases:
Endless Forms & Deadlines: Patients must provide new documentation at short notice.
Auto-Expiration Policies: A missed deadline results in “coverage lapse.”
Minimal Staff Guidance: Helplines with multi-hour wait times discourage follow-up.
These administrative hurdles disproportionately impact disabled, low-income, and elderly patients, who often lack digital access, flexible work schedules, or caregiver support to navigate the system.
Example: A construction worker with limited internet access misses a renewal letter for Medicaid. His coverage is quietly dropped. When he attempts to reapply after his condition worsens, he faces weeks of delays—turning what should have been a minor intervention into an emergency.
These tactics reflect a larger pattern of withholding abundance—where resources exist but are strategically kept out of reach to maximize profit-driven efficiency.
c. Why This Remains Invisible
Unlike outright denial, Actuarial Medicine leaves no paper trail. Patients who abandon the process:
Aren’t counted in rejection statistics.
Don’t appear in readmission rates.
Never factor into hospital cost reports.
Analogy: If a teacher removes the lowest-scoring students before the final exam, the class average rises—not because they performed better, but because the worst-off students were erased from the dataset.
This is why hospitals boasting about low costs and short stays should trigger scrutiny: Who is missing from the data? Who never received care in the first place?
The Fallout: Delayed Care Becomes Catastrophe
Deferring Care Until It Becomes a Crisis
By quietly discouraging borderline cases, hospitals shift costs to later, more expensive interventions. A patient who could have been treated early for $2,000 might end up in the ER months later with life-threatening complications, costing $25,000.
Hospitals celebrate the short-term savings.
Public hospitals, emergency rooms, and taxpayers absorb the long-term costs.
This form of cost deferral mirrors the logic of residency labor exploitation, where institutions rely on temporal injustice to extract the most value while offloading long-term burdens elsewhere.

The Heaviest Burden Falls on Marginalized Groups
Actuarial Medicine exacerbates systemic health inequities. Patients most likely to be filtered out include:
Disabled & Elderly Patients: Higher likelihood of chronic conditions and multiple comorbidities.
Low-Income & Uninsured Patients: More likely to face coverage lapses and administrative friction.
Racial & Ethnic Minorities: Algorithmic bias may disproportionately label certain zip codes or demographics as high-cost risks.
Example: A predominantly Black neighborhood reports three times the rate of “incomplete” admissions compared to wealthier areas. Officially, “They didn’t comply with paperwork.” The reality? Administrative hurdles were selectively applied to weed out costly patients.
This exclusionary design aligns with the architecture of harm in healthcare—where systems that claim neutrality are structured to disproportionately burden the most vulnerable.
What Needs to Change?
a. Public “Exclusion Logs”
Hospitals should be required to publish how many patients “timed out” due to coverage or bureaucratic hurdles.
Breakdowns should include demographics to highlight systemic biases.
b. Algorithmic Transparency & Audits
Independent regulators should audit hospital AI systems to examine whether risk-scoring disproportionately flags certain groups.
Hospitals should be required to disclose triage criteria instead of hiding behind “trade secrets.”
c. Financial Incentives That Reward Complex Care
Shift reimbursement models to incentivize early intervention, rather than penalizing complex cases.
Eliminate profit motives for avoiding high-need patients.
d. Redefining Success Metrics
Instead of celebrating shorter hospital stays or lower costs per patient, hospitals should be judged on:
How many borderline patients actually receive timely intervention.
How many staff hours and empty wards remain underutilized while patients are turned away.
e. Legal & Advocacy Pathways
If exclusion disproportionately impacts disabled, low-income, or racial groups, civil rights lawsuits may be warranted.
Community groups can track “missing” admissions, forcing local hospitals to disclose how many patients were funneled out before care.
Counting the Uncounted
Actuarial Medicine is illusory efficiency. It is a hidden rationing system that discards those deemed too expensive.

If we want a truly ethical and effective healthcare system:
We must count everyone who seeks care—not just those who survive administrative triage.
We must expose quiet exclusion—ensuring that invisible patients become visible in the data.
We must redesign incentives to prioritize care over cost optics—because abandoning complex patients is not a savings. It’s a human and economic crisis deferred.
It’s time to stop mistaking exclusion for efficiency—and start demanding a system that serves all patients, not just the cheapest ones.